Our office will be closed from 9/25 – 10/23. Any orders placed during this time will be shipped upon return by 11/1/23.
by Bill Perkins
Published on April 30, 2020

Published By
Earl Smith
Principal at Brooks Advisory Partners
Many and varied are the superlatives attached to the global COVID-19 pandemic. The response by officials in the United States has been robust in light of early model estimates of potential deaths counted in the millions. References to the 1917 Spanish flu have been numerous and quarantine / physical distancing orders have largely been predicated on the specter of mass death nationwide and globally if the citizenry failed to comply. Maintaining a broad and level-headed perspective of our collective condition has been, for many, especially challenging. Fortunately, ongoing data collection and reporting by various U.S. health agencies may shed light on how COVID-19 compares with past and ongoing healthcare issues in the United States. Consider the following.
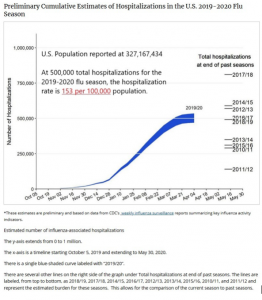
HOSPITALIZATION RATES
Centers for Disease Control (CDC) data for annual hospitalization rates due to flu in the United States due suggest the 2019-2020 season is near the median value over the last ten years (https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm). The hospitalization rate estimated by CDC for 2019-2020 is approximately 153 per 100,000 population in the U.S. For reference, hospitalizations during the 2017-2018 season were 810,000 or approximately 240 per 100,000 population.
Laboratory-confirmed COVID-19 hospitalizations, reported by CDC as of April 18, 2020, are at a rate of 29 per 100,000 population in the U.S.
(https://gis.cdc.gov/grasp/covidnet/COVID19_3.html).
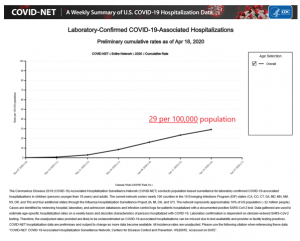
The combination of flu season hospitalizations (153 per 100,000) plus COVID-19 hospitalizations per (29 per 100,000) add to a combined rate of 182 per 100,000. A hospitalization rate of 182 per 100,000 would be approximately 76% of the peak hospitalization rate for flu alone managed during the 2017-2018 season. COVID-19 hospitalization rates to-date do not appear to represent an exceptional challenge to hospital capacity utilization in the aggregate.
DEATH RATES
COVID-19 has, however, been described as especially lethal and more deadly than other diseases. CDC and the National Center for Health Statistics (NCHS), for the period February 1 through April 25, report a total of 33,513 confirmed COVID-19-related deaths. COVID-19-related deaths are included in the 706,401 total U.S. deaths from all causes during this same 84-day period. On a daily basis, 8,410 deaths occurred from all causes including 399 deaths per day associated with COVID-19. For reference, pneumonia deaths (not involving COVID-19) during this period were 737 per day. Total confirmed COVID-19 deaths during this reporting period were 4.7% of deaths from all causes.
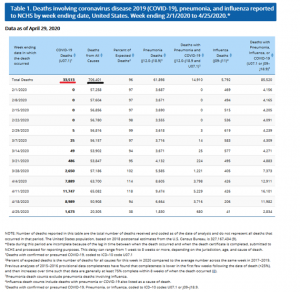
Data shown above for COVID-19 deaths clearly show a peak in deaths during the week of April 11 and a decline in each of the two weeks thereafter.
DEATHS DUE TO COVID-19 vs. OTHER CAUSES
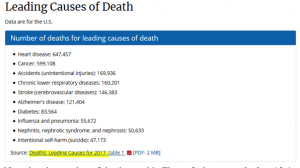
Regarding COVID-19 death rates compared to other diseases, CDC reports death rates for all causes and then by specific causes in descending order in Figure 2 below. Data are presented for both 2017 and 2018. Final data for 2019 remains pending. (https://www.cdc.gov/nchs/products/databriefs/db355.htm). Deaths reported by Johns Hopkins' COVID-19 Dashboard on April 29 imply a COVID-19 ranking of 8th most lethal of U.S. diseases.
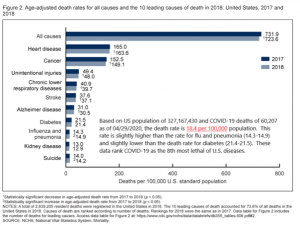
Actual death counts during 2017 are also shown below for reference (https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm):
Note that the number of deaths used in Figure 2 above to calculate 18.4 deaths per 100,000 is a higher, but as yet unconfirmed, death count of 60,207 reported by the Johns Hopkins COVID-19 Dashboard on April 29 at 2:29 p.m.
(https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6).
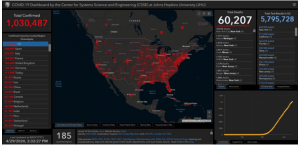
The deaths reported daily by the Johns Hopkins COVID-19 Dashboard may or may not ultimately be confirmed as COVID-19 deaths when reported by NCHS in subsequent updates to the reports shown in Table 1 above.
POPULATION MOST AT RISK
CDC reports 706,401 COVID-19 deaths during the 84-day period referenced in Table 1 above. Data indicate that of the 33,513 COVID-19 deaths during this period, 80% (26,667) were 65 years of age and older (https://www.cdc.gov/nchs/nvss/vsrr/COVID19/index.htm). The age bracket from 15-54 years of age accounted for less than 8% of total COVID-19 deaths (2,638) during the period.

CONCLUSIONS
While this has been an especially difficult and disruptive period as the U.S. and the rest of the world has dealt with the COVID-19 pandemic, data reported by U.S. health agencies confirm reasons to be encouraged. These include the following:
1. Hospital capacity for handling the COVID-19 pandemic has been sufficient and is expected to remain so based on current rates of infection. Increased availability of ventilators is also supportive.
2. COVID-19 may rank 8th among leading causes of death in the United States. This is slightly higher than seasonal flu and somewhat lower than the rate of deaths due to diabetes.
3. 80% of COVID-19 deaths have been individuals 65 years of age and older. Prime working-age individuals ages 25-54 have accounted for less than 8% of COVID-19 deaths.
4. Citizens of the United States successfully manage risks in their daily lives. Returning to a normal family/work/worship/community routine is both warranted and overdue.
THE PRICE ALREADY PAID
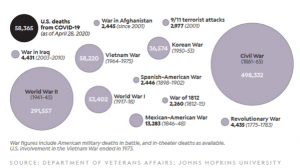
Caring U.S. citizens are rightfully concerned for the health and welfare of their fellow countrymen. The collective and individual acts of service and sacrifice taken by the American people during the COVID-19 pandemic have been beneficial and saved lives. But lest we forget, many hundreds of thousands of Americans before us laid down their own lives and paid the full measure of devotion for the life and liberty of these our United States.
We mourn the loss of each victim of the virus that has recently afflicted our world and our country. But let us resist with all vigor anyone who would seek to use this pandemic as an excuse to take our rights and liberties casually in pursuit of their own selfish personal or political ambitions. We live in the land of the free and the home of the brave. Therefore, let us live bravely in a manner worthy of those whose ultimate sacrifice gained our freedom and seek to preserve it for our posterity.